CRS is a complex inflammatory syndrome of the nose and paranasal sinuses, with three major subtypes: CRSsNP, CRSwNP, and AFRS. Diagnosis requires both objective structural evidence of sinus inflammation (CT or endoscopy) and ≥2 cardinal symptoms for ≥12 weeks (nasal congestion, facial pain or pressure, nasal drainage, and absent or reduced smell). Preliminary workup involves aeroallergen testing with other ad-hoc tests. First-line management includes trigger avoidance, saline rinses, and INCS; failure of medical therapy may need ENT surgery. Biologics such as dupilumab are very effective for CRSwNP, and are indicated for refractory/severe presentations.
onset
duration
Cardinal symptoms: [nasal congestion/fullness | facial pain/pressure/fullness | anterior or posterior nasal drainage (?purulent) | hypo/anosmia]
Other symptoms: [change in voice | cough | headache | fatigue/disruption of sleep | halitosis/dental pain | ear pain/fullness]
CT/ENT before? Known nasal polyps?
? asthma/COPD, AR, CF, NERD/ASA sensitivity, recurrent infect, EtOH induced worsening of upper airway disease, impaired cilia(CF, PCD), smoking, pollution, occupational exposure, nasal anatomic variations, vasculitis
Treatment trials
SNOT-22 Score
# Chronic rhinosinusitis (CRS) wNP sNP AFRS
Their clinical picture is suggestive of CRS, an inflammatory syndrome defined by objective structural evidence of sinus inflammation and ≥2 cardinal symptoms (nasal congestion, facial pain/pressure, anterior/posterior nasal drainage, absent/reduced smell) ≥12 weeks. While chronic, regular pharmacotherapy can usually control symptoms well.
Recommendations:
* CT sinuses (non-contrast) vs ENT referral
* SPT for common aeroallergens
* Ad-hoc testing: ie. B-cell immunodeficiency workup in setting of suspicious symptoms / acute recurrent sinusitis
> High volume nasal saline rinses, avoidance of triggers
> INCS + treatment of any underlying causes
> Consider short course prednisone for symptom management (most evidence for CRSwNP or AFRS)
> Consider biologics for CRSwNP if severe/failed first-line therapy
Follow-up: ~3-4 months
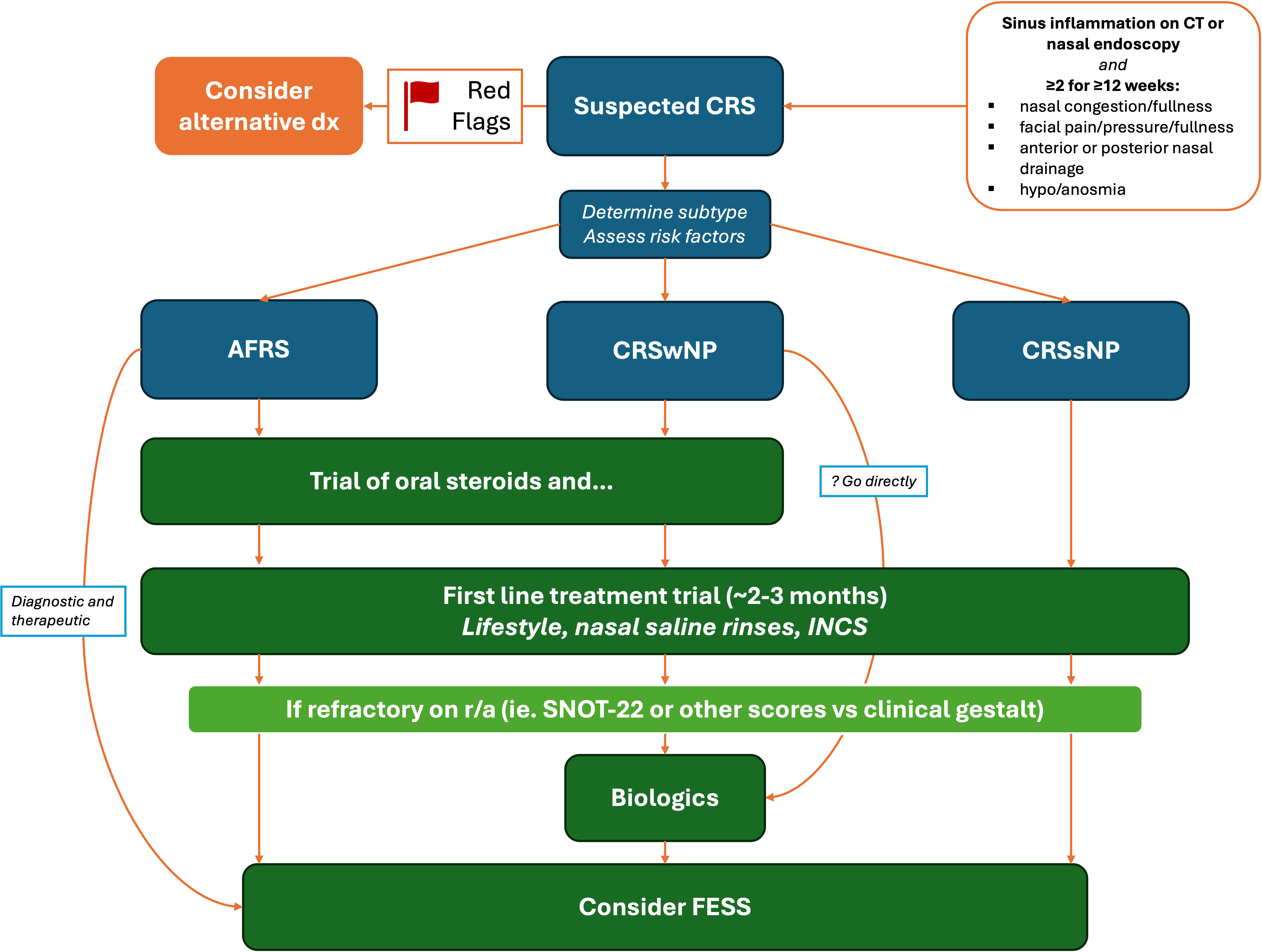
Summary diagram
Definitions
AFRS: allergic fungal rhinosinusitis
CRS: chronic rhinosinusitis
CRSsNP: chronic rhinosinusitis without nasal polyps
CRSwNP: chronic rhinosinusitis with nasal polyps
FESS: functional endoscopic sinus surgery
NERD: NSAID exacerbated respiratory disease
OMC: Ostiomeatal complex
Diagnostic criteria (multiple exist)
Requires both ≥2 key symptoms for ≥12 weeks AND objective structural evidence of sinus inflammation:orlandi_international_2021, hamilos_chronic_2011
Key symptoms - at least 2 for at least 12 weeks
Nasal obstruction or congestion
Facial pain, pressure, or fullness
Nasal discharge (rhinorrhea or post-nasal drip)
Absent or decreased sense of smell
Cough (in Pediatric CRS)
Objective sinus inflammation
This is done through either:
CT sinuses (non contrast) – will visualize sinus mucosal thickening, opacification (plain XR is not sensitive), OR
Direct visualization with nasal endoscopy
Requires both ≥2 key symptoms for ≥8-12 weeks and at least 1 objective finding on endoscopy or CT scan: desrosiers_canadian_2011
Key symptoms
Facial congestion/fullness
Facial pain/pressure/fullness
Nasal obstruction/blockage
Purulent anterior/posterior nasal drainage (discharge may be nonpurulent, non discolored)
Hyposmia/anosmia
≥2 key symptoms for ≥12 weeks (at least one from a 'major' criteria) and at least 1 objective finding on endoscopy or CT scan: fokkens_european_2020
Major symptoms
Nasal blockage / obstruction / congestion
Nasal discharge (anterior / posterior nasal drip)
Minor symptoms
Adult: facial pain/pressure, OR reduction or loss of smell
Peds: facial pain/pressure, OR cough
≥2 key symptoms for ≥12 weeks and at least 1 objective finding on endoscopy or CT scan: rosenfeld_clinical_2015
Key symptoms
mucopurulent drainage (anterior, posterior, or both),
nasal obstruction (congestion)
facial pain-pressure-fullness
decreased sense of smell
Epidemiology and classifications
Overall epidemiology
Canadian prevalence ~2-15% chin_diagnosis_2025; CRSsNP > CRSwNP >> AFRS
Adults and pediatrics affected, mean diagnosis age ~39, females slightly > males chin_diagnosis_2025, lee_acaai_2024
Associated with increased healthcare costs + decreased QoL
Often symptoms are long-standing before presenting to medical attention, given low-grade severity
Other non-specific symptoms include ear fullness, headache, fatigue, altered taste, cough
CRSsNP
Most common (~⅔ of cases)
Likely link to allergies, infections, irritants, etc.
Classically thick and mucopurulent anterior/posterior nasal discharge predominant, less hypo/anosmia than CRSwNP
May have persistent symptoms with occasional flares
CRSwNP
Polyps are soft, usually bilateral avascular eosinophil-rich growths that most commonly grow from the ethmoid sinuses
Compared with CRSsNP, stronger association with asthma (~25% of patients), AFRS, NERD chin_diagnosis_2025
Often stuffy nasal quality to voice
AFRS
Inflammation from hypersensitivity to usually commensal fungi
More often in younger immunocompetent individuals in hot/humid climates (moreso in the US) and low SES; associated with polyposis hamilos_chronic_2011, lee_acaai_2024
Classically peanut-butter like mucus, very thick and tenacious
Specific criteria: ALL of
CRS symptoms, Type 1 hypersensitivity to fungi confirmed by history, skin test, or serology, typical CT findings, Eosinophilic mucin with non-invasive fungal hyphae, absence of immunodeficiency, uncontrolled diabetes lee_acaai_2024
FYI: A new classification system?
In 2020 a new classification system beyond sNP/wNP/AFRS was proposed based on primary vs secondary causes, and localization/type of inflammation (local vs diffuse; TH2 skewed vs non-TH2). grayson_contemporary_2020
Note that not all guidelines / position statements use this classification. Read the referenced JAMA article if you’re interested in learning more :)
flowchart LR
A["Primary CRS"] --> B["Localized
(unilateral)"]
A --> C["Diffuse
(bilateral)"]
B --> D["Type 2"]
B --> E["Non-type 2"]
C --> F["Type 2"]
C --> G["Non-type 2"]
D --> H["AFRS"]
E --> I["OMC
Isolated frontal
Isolated sphenoid"]
F --> J["CCAD
eCRS
AFRS"]
G --> K["Non-eCRS
Poor corticosteroid response
Older or smoker"]
flowchart LR
A["Secondary CRS"] --> B["`Localized
(unilateral)`"]
A --> C["`Diffuse
(bilateral)`"]
B --> D["`Local
pathology`"]
C --> E["`Mechanical
(mucociliary)`"]
C --> F["`Inflammatory
(autoimmune)`"]
C --> G["`Immunity
(immunodeficiency)`"]
D --> H["`Odontogenic
Fungal ball
Tumor`"]
E --> I["`PCD
CF`"]
F --> J["`GPA
EGPA`"]
G --> K["`Selective IgA
deficiency
CVID
Diabetes`"]
Unexplained weight loss, recurrent fevers, night sweats
Pathophysiology and risk factors
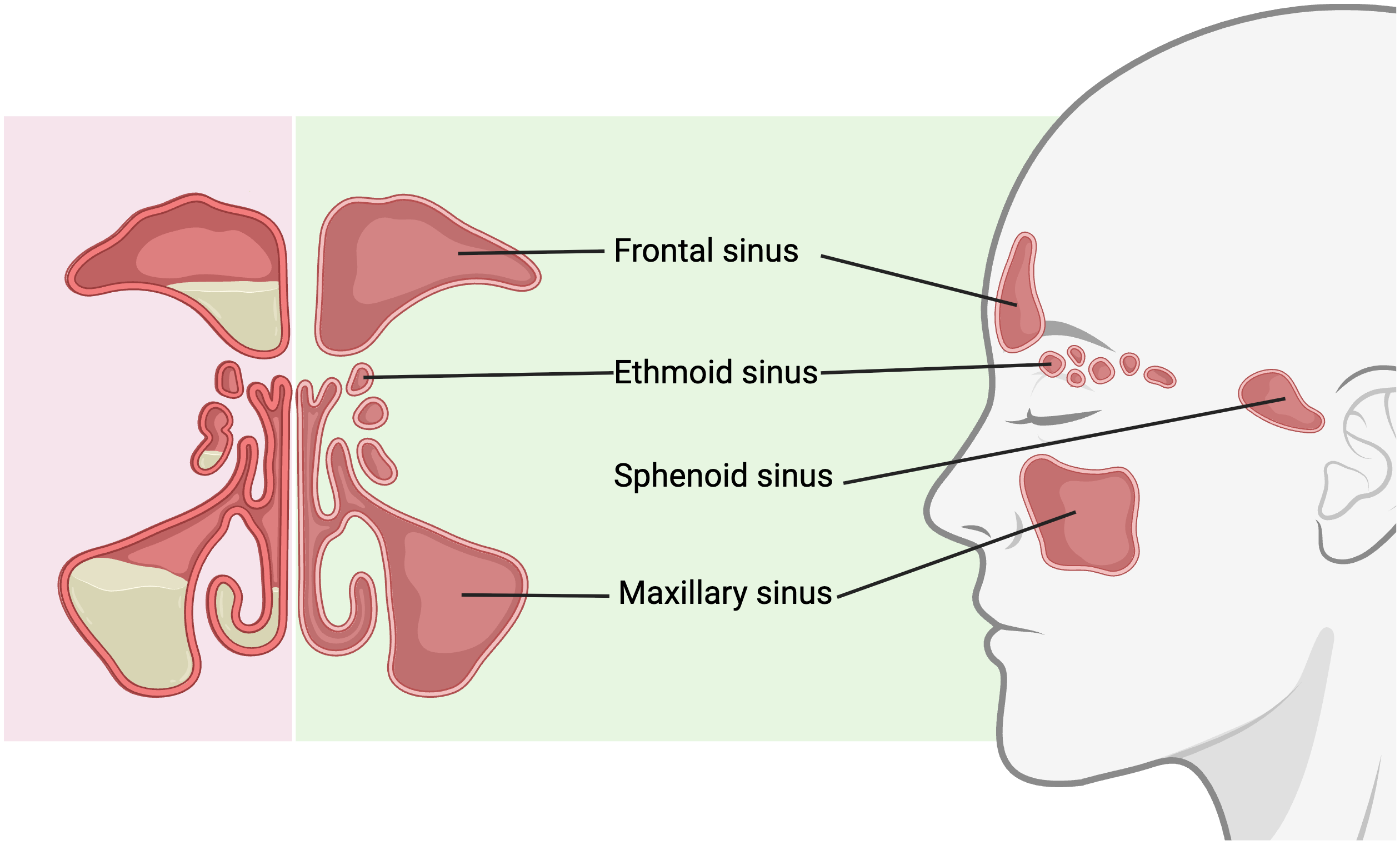
Red = inflamed sinuses, green is happy :) Created in https://BioRender.com
The sinuses
Sinuses lined by thin mucosal layer with cilia and goblet cells
A key ostium (a connection from sinus into the nose) is the OMC
The chronically inflamed sinuses
Exact cause not understood for any subtype of CRS, but overall CRS is more inflammatory > infectious
Likely combination of physical/environmental insults, hypersensitivity, microbial pathogens, and structural abnormalities that ultimately lead to sinus mucosal dysfunction/inflammation, poor drainage/aeration, and resultant symptoms
For AFRS, common organisms: Bipolaris, Curvularia, Alternaria, Rhizopus, Drechslera, Helminthosporium, Fusarium, and Aspergillus lee_acaai_2024
Exaggerated TH2 response and very thick mucous forms
Predisposing conditions/risk factors to assess for ALL CRS
Allergic rhinitis (common culprits: dust mites, pets, molds, cockroaches); typically secretions are more clear/thin
Humoral deficiency - often recurrent purulent infection
HIV
Vasculitis
Pre-existing structural issues (ie. deviated septum): may predispose, but by themselves are a very uncommon cause. Weak evidence
Investigations
No standard panel of tests. However, consider ad-hoc testing such as:
SPT / sIgE (most likely you will do this consistently)
Quantitative immunoglobulins and other humoral deficiency workup
Ciliary function testing
CF testing
NERD testing
Asthma testing
Management
Goal of treatment is usually NOT curative
Goals are symptom control through reduction of inflammation and improvement of sinus patency.
THE BRASS TACKS
Determine subtype of CRS, consider CT sinus and involvement of ENT colleagues for endoscopic assessment & consideration of early management
First-line treatment trial (unless AFRS => likely early FESS + altered first-line) for at least 2-3 months, + treatment of any underlying risk factors (ie. AR, GERD, CF, immunodeficiency)
Monitor treatment either through scores (SNOT-22) vs gestalt clinical judgement
Specific subtype treatment (ie. biologics for CRSwNP if patient qualifies)
FESS if medically refractory
First line treatment
Treat any underlying risk factors (who knew?)
Lifestyle
Avoidance of environmental triggers/insults/allergens
High volume nasal saline rinses/irrigation (OTC, rinses > sprays), at least 200 mL per side chong_saline_2016. Can improve penetration/efficacy of other topicals if used beforehand
Examples: neti pot, squeeze bottles, etc. Must be STERILE saline (boiled/distilled water)
INCS
Multiple delivery methods, most common in Canada are spray and rinses; widely available but very common operator misuse with sprays (see how to use here)
Takes 8-12 weeks to have maximal effect
Minimal concern for long-term side effects, ie. adrenal insufficiency
ExRx: Nasonex 2 sprays BID
Rx
Mometasone furoate
(INCS)
Brand Names:
Nasonex,
Sinuva
Routes:
nasal spray (50mcg)
MoA:
Steroid, topical
Half-life:
~5.8 hours
Time to peak action:
While monograph says ~12 hours, maximal effect requires 2-4 weeks of use
Doses:
AR:
1-4 sprays (50mcg per spray) EN OD (ages ≥12)
1 spray (50mcg per spray) EN OD (ages 3-11)
CRS:
1-2 sprays (50mcg per spray) EN BID (ages ≥12)
Coverage:
ON (ODB)
Age Group:
ages ≥3
Pregnancy:
Maybe OK, but no adequate or well-controlled studies in pregnant or nursing women
Contraindications:
Hypersensitivity, acute bacterial sinus infection without antibiotics
Common SEs:
For adults: headache 8%[D], 6%[P]; epistaxis 8%[D], 5%[P], pharyngitis 4%[D], 3%[P]. For 3-11, all comparable to placebo
Severe SEs:
All very rare (<1%): liver enzyme elevation
Table adapted from Fowler and Sowerby (2021)fowler_using_2021
Consider involving ENT for endoscopic assessment and consideration of early surgical management
Antibiotics
May consider for acute flares. Most common organism is S. aureus
CAUTION: this is not a routine treatment and there is poor quality evidence it has benefit fokkens_european_2020: exercise antibiotic stewardship :). If requiring multiple courses or known resistant bugs => CULTURE first
ExRx: clavulin 875 mg twice daily for 10 d, moxifloxacin 400 mg PO x10 if penicillin allergic
PEARLS
Empiric treatment without imaging/endoscopy?
While technically imaging or endoscopy is needed to formally diagnose CRS, if the clinical history is otherwise consistent, empiric first-line treatments are often trialed for a few months first before those tests (unless you suspect AFRS or CRSwNP).
Oral steroids for quick temporary relief
You may see oral corticosteroids used up-front for severely symptomatic cases, but more commonly for CRSwNP and AFRS.
How is treatment monitored?
In an ideal world, with regular use of validated scores such as SNOT-22 or SNOT-20 (higher score = worse QoL). However, it is not uncommon to see mainly gestalt (and therefore variable) assessments of symptom control.
SNOT-22 SCORE
CRSsNP specific treatment
Trial first-line treatment. You may see the concept of “up-front intensive treatment”, where they get oral steroids + antibiotics to obtain good symptom control hamilos_chronic_2011, though much weaker evidence compared to CRSwNP or AFRS
Look for risk factors (ie immunodeficiency, CF) especially if refractory to treatment
Surgery last line
No biologics yet
DEEP-DIVE: INCS sprays in CRSsNP
Bottom line: while recommended and common, evidence of benefit for INCS sprays in CRSsNP is actually unclear/sparse, though low-harm
EPOS 2020 – symptom score benefit in CRS was lower than CRSwNP; only 5 RCTs with CRSsNP listedfokkens_european_2020
Topical steroids for chronic rhinosinusitis without nasal polyps: A systematic review and meta-analysisbhat_topical_2024
Only 5 RCTs used sprays, but there was: 1) large variability on how symptoms and ‘response to treatment’ were assessed 2) No RoB was reported for each individual trial 3) relatively small overall sample size for outcomes such as symptom scores
Our opinion of this review: low quality of evidence (GRADE; unreported RoB, indirect/variable outcome assessment)
CRSwNP specific treatment
Trial first-line treatment + often a short course of oral steroids
Oral steroids = rapid temporary relief that fades by a few months head_shortcourse_2016; must consider significant S/E profile
ExRx: prednisone 30 mg OD x7d chin_diagnosis_2025; note that there is no consensus/consistent dose between trials
DEEP-DIVE: INCS in CRSwNP
Bottom-line: there is generally low quality evidence that INCS compared to placebo improves symptoms and QoL without significant side effects, though specifics vary by delivery system
The Joint Task Force on Practice Parameters GRADE guidelines for the medical management of chronic rhinosinusitis with nasal polyposisrank_joint_2023
Note: sprays are cheap and widely available; EDS $$$$$
Patient-Important outcomes
Critical Outcomes
Important Outcomes
HR-QoL SNOT-22 (0-120)
Symptoms (Nasal Obstruction) VAS (0-3)
Smell UPSIT (0-40)
Rescue Surgery
Severe Adverse Events
Any Adverse Events
Placebo (reference)
-19.41
-0.56
3.54
13.58%
2.76%
28.66%
Spray
-3.62 (-9.27, 2.04)
-0.51 (-0.61, -0.41)
3.24 (2.05, 4.42)
-10.7% (-13%, -2.1%)
-0.1% (-0.8%, 0.5%)
2.7% (-0.7%, 6.1%)
Rinse
-6.83 (-11.94, -1.71)
-0.21 (-0.76, 0.33)
2.77 (-0.84, 6.39)
0.00% (-4.3%, 4.2%)
-0.6% (-8.5%, 7.3%)
EDS
-7.86 (-14.64, -1.08)
-0.35 (-0.51, -0.18)
4.10 (1.69, 6.52)
-4.3% (-6.9%, -0.9%)
-1.0% (-3.3%, 1.3%)
2.9% (-14.8%, 20.7%)
High Dose Spray
-7.46 (-25.20, 10.6)
-0.51 (-0.85, -0.16)
-1.0% (-11.6%, 9.6%)
1.8% (-11.8%, 15.4%)
Classification of the intervention (color)
GRADE CoE (Shading)
Among most beneficial
Among least beneficial / no clear effect compared to placebo
High/Moderate CoE (Solid)
Among most harmful
No data (blank)
Low/Very Low CoE (Shaded)
At any point biologics can technically be considered, especially if high baseline severity or refractory to other medical therapy; greatest positive effect on QoL outcomes rank_joint_2023
Three options: dupilumab (2024 monograph states adults, but studied in ≥12 yo for other indications), omalizumab (adults), mepolizumab (adults) (***tezepelumab (Tezspire) is coming soon! Update TBD)
All overall have excellent side effect profile
Cost/insurance prohibitive
Unclear on: long-term side effects, duration of treatment, predictive patient factors for most benefit
. S/E profile similar to placebo but classically conjunctivitis, eosinophilia, injection site reactions
DEEP-DIVE: Biologics in CRSwNP
Bottom-line: moderate/high quality evidence supporting large effect sizes of biologics in addition to INCS, with minimal side effects compared to placebo. Dupilumab had the largest effect sizes across multiple outcomes
The Joint Task Force on Practice Parameters GRADE guidelines for the medical management of chronic rhinosinusitis with nasal polyposisrank_joint_2023